
The dysplastic nevus: a diagnosis that tells you less than it seems
A common dermatopathology report, the noise in the grade, and what the evidence supports doing

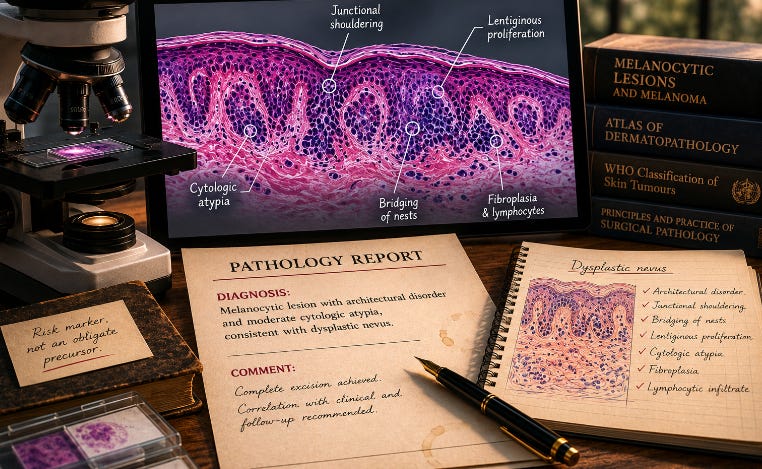
A patient sits across from their dermatologist holding a pathology report. It reads: melanocytic lesion with architectural disorder and moderate cytologic atypia, consistent with dysplastic nevus. The question is always the same: what do we do with this?
It is a fair question. The diagnosis is common. In any busy dermatopathology practice, dysplastic nevi are among the most frequently reported melanocytic lesions. And the answer, in most cases, is less clear than that frequency implies.
What the histology actually describes
A dysplastic nevus is defined histologically by two things: architectural disorder in the junctional component, and cytologic atypia. The architectural features include junctional “shoulders” extending beyond the dermal part of the lesion, bridging of nests between rete ridges, lentiginous melanocyte proliferation at the periphery, fibroplasia in the superficial papillary dermis, and a patchy lymphocytic infiltrate (Duffy & Grossman, 2012; Menzinger et al., 2025). Clinically, these lesions tend to be larger than ordinary nevi, asymmetric, with irregular borders and color variation. Those features overlap with both benign nevi and early superficial spreading melanoma.
The 2018 WHO classification placed dysplastic nevi within a two-tier grading system: low-grade and high-grade (Ferrara & Argenziano, 2021). The intention was to reduce the intermediate categories that nobody quite knew what to do with.
In practice, the grading remains the central problem.
The reproducibility problem
Pathologists do not reliably agree on this diagnosis, particularly on the grade. Every clinician who sends tissue for melanocytic evaluation should know that.
In the classic interobserver studies, agreement was unreliable across the board. Grading kappa values among experienced dermatopathologists ranged from 0.38 to 0.47 (Duncan et al., 1993); recognition agreement ranged from 0.32 to 0.71 across observers (Duray et al., 1992). Applying the 2018 WHO criteria improved standardization in principle; in practice, a study applying those exact criteria to a series of cases found only fair multirater agreement (κ = 0.40) (Ulgen et al., 2021). A Norwegian reassessment of melanocytic lesions excised across two different time periods found that agreement for the category “irregular/dysplastic nevus” was approximately 29%, and for “nevus with severe atypia” approximately 28% (Gjersvik et al., 2022). A 2025 multicenter study published in Nature Communications confirmed what many dermatopathologists already knew from case conferences: discordance in this diagnostic space is substantial, even among experienced specialists (Haggenmüller et al., 2025).
A large tertiary-center study found overall concordance of 72% across all melanocytic diagnoses, substantially lower than for unambiguous melanoma (Ronen et al., 2021). For clear-cut melanoma and ordinary common nevi, agreement is high. For the lesions between those poles, including moderately dysplastic nevi, it drops considerably.
The practical implication is uncomfortable but important: the same slide, seen by two competent pathologists, may receive a different grade. Occasionally a different diagnosis entirely. This is not individual failure. It reflects the biological reality that the morphological features used to grade atypia sit on a continuum, without a reliable histological bright line.
What the biology says
The current evidence, consolidated across multiple independent lines of research, supports viewing dysplastic nevi primarily as risk markers, not obligate precursors to melanoma (Duffy & Grossman, 2012; Menzinger et al., 2025; Ferrara & Argenziano, 2021; Wiedemeyer et al., 2021). Most melanomas arise de novo, not from pre-existing nevi. Some arise from common nevi or dysplastic nevi, but the per-lesion risk is low. Having multiple dysplastic nevi, or having them in a patient with a personal or family history of melanoma, increases overall risk. A solitary mildly dysplastic nevus in a low-risk patient is a different clinical situation.
The most pointed position in the literature is Bernard Ackerman’s, articulated posthumously by Hurwitz and Tavel (2015): the diagnosis of dysplastic nevus is “mythical” and its clinical consequences are “untoward”, creating patient anxiety and surgical overtreatment without evidence of benefit, based on histological criteria too imprecise to justify the label. Ackerman was not universally right, and this view has not prevailed. But the argument belongs in the clinical conversation, not on the margins of it.
What to do — the management question
For high-grade dysplasia: most authors and the WHO recommend complete excision. The overlap with melanoma in situ at this end of the spectrum, combined with the diagnostic discordance precisely at that boundary, makes a conservative surgical approach reasonable (Duffy & Grossman, 2012; Menzinger et al., 2025; Ferrara & Argenziano, 2021). Margins of 2 to 3 mm are generally sufficient. A 2020 retrospective series of 426 severely dysplastic nevi re-excised with exactly those margins found no upstaging to melanoma, no local recurrences, and very low rates of residual dysplastic tissue when the initial biopsy had already removed the bulk of the lesion histologically (Soleymani et al., 2020). The data do not support wider excision as a default.
For low-grade and moderate dysplasia with complete initial excision: routine re-excision is not supported by the available evidence (Duffy & Grossman, 2012; Soleymani et al., 2020; Ferrara & Argenziano, 2021). The reflex to re-excise every lesion reported as dysplastic generates surgical morbidity without demonstrated clinical benefit. A complete excisional biopsy with clear margins is, in most cases, sufficient treatment.
What matters more than re-excision in the mild-to-moderate group is follow-up. A patient with multiple dysplastic nevi warrants annual total-body skin examination by a dermatologist who knows their baseline. A patient with a single mildly dysplastic nevus, fully excised, with no other risk factors, warrants explanation and surveillance, not revision surgery.
What a patient should conclude
If you have received this diagnosis: it is not a cancer diagnosis. The word “dysplastic” is alarming in a way that is not proportional to what the diagnosis usually means. For most lesions in this category, the per-lesion risk of progression to melanoma is low.
The diagnosis suggests your skin warrants monitoring. This particular lesion is unlikely to become dangerous, but lesions with these features place you in a group for whom ongoing dermatological surveillance is appropriate. That is not the same as having a precancer.
Two questions worth asking your clinician: was the excision histologically complete, and what grade of atypia was reported? If the answers are yes and mild-to-moderate, the most defensible next step is surveillance. If the grade is high, or the margins were incomplete, re-excision is worth discussing.
The diagnostic problem is not going away
AI-assisted image analysis, molecular adjuncts (p16 immunohistochemistry, 9p21 FISH), and standardized reporting schemas such as MPATH-Dx are all being used to reduce the uncertainty in this diagnostic space (Barnhill et al., 2023; Vergara et al., 2025). They help, in selected cases. They have not resolved the fundamental issue: morphological grading of melanocytic atypia is a judgment, and judgments vary.
The honest position is that the dysplastic nevus diagnosis is more reliable at the poles, clearly low-grade or clearly high-grade, than in the middle, which is precisely where most clinically consequential uncertainty sits.
Understanding that is more useful than either dismissing the diagnosis or acting on it as though the grade were a precise measurement. It is not.
This post is educational. It does not refer to any real patient or clinical case. If you have received a pathology report and have questions about it, speak to the physician or pathologist who issued the report.
Disclosures. I am a histopathologist at AML (Antwerp) and full professor of pathology at the University of Antwerp. I have no financial interest in any diagnostic technology or vendor mentioned in this post.
References
Barnhill, R.L., Elder, D., Piepkorn, M., et al. (2023). Revision of the Melanocytic Pathology Assessment Tool and Hierarchy for Diagnosis Classification Schema for Melanocytic Lesions: A Consensus Statement. JAMA Network Open, 6(1), e2250613. https://doi.org/10.1001/jamanetworkopen.2022.50613
Duncan, L.M., Berwick, M., Bruijn, J.A., Byers, H.R., Mihm, M.C., & Barnhill, R.L. (1993). Histopathologic recognition and grading of dysplastic melanocytic nevi: an interobserver agreement study. Journal of Investigative Dermatology, 100(3), 318S–321S. https://doi.org/10.1111/1523-1747.ep12470215
Duffy, K., & Grossman, D. (2012). The dysplastic nevus: from historical perspective to management in the modern era: part I. Journal of the American Academy of Dermatology, 67(1), 1.e1–16. https://doi.org/10.1016/j.jaad.2012.02.047
Duffy, K., & Grossman, D. (2012). The dysplastic nevus: from historical perspective to management in the modern era: part II. Journal of the American Academy of Dermatology, 67(1), 19.e1–12. https://doi.org/10.1016/j.jaad.2012.03.013
Duray, P., DerSimonian, R., Barnhill, R., Stenn, K., Ernstoff, M., Fine, J., & Kirkwood, J. (1992). An analysis of interobserver recognition of the histopathologic features of dysplastic nevi from a mixed group of nevomelanocytic lesions. Journal of the American Academy of Dermatology, 27(5 Pt 1), 741–749.
Ferrara, G., & Argenziano, G. (2021). The WHO 2018 Classification of Cutaneous Melanocytic Neoplasms: Suggestions From Routine Practice. Frontiers in Oncology, 11. https://doi.org/10.3389/fonc.2021.675296
Gjersvik, P., Veierød, M., Thompson, A., Grzyb, K., Lilland, K., Vazov, N., Roscher, I., & Bassarova, A. (2022). Histopathologic reassessment of melanoma and other melanocytic skin lesions excised in 2009 and 2018–2019. Tidsskrift for den Norske laegeforening, 142(15). https://doi.org/10.4045/tidsskr.22.0204
Haggenmüller, S., et al. (2025). Discordance, accuracy and reproducibility study of pathologists’ diagnosis of melanoma and melanocytic tumors. Nature Communications, 16. https://doi.org/10.1038/s41467-025-56160-x
Hurwitz, R., & Tavel, M. (2015). The mythical concept and untoward consequences of a diagnosis of dysplastic nevus: an overdue tribute to A. Bernard Ackerman, MD. Dermatology Practical & Conceptual, 5, 31–34. https://doi.org/10.5826/dpc.0501a05
Menzinger, S., Merat, R., & Kaya, G. (2025). Dysplastic Nevi and Superficial Borderline Atypical Melanocytic Lesions: Description of an Algorithmic Clinico-Pathological Classification. Dermatopathology, 12. https://doi.org/10.3390/dermatopathology12010003
Ronen, S., Al-Rohil, R., Keiser, E., et al. (2021). Discordance in Diagnosis of Melanocytic Lesions and Its Impact on Clinical Management. Archives of Pathology & Laboratory Medicine. https://doi.org/10.5858/arpa.2020-0620-oa
Soleymani, T., Swetter, S., Hollmig, S., & Aasi, S. (2020). Adequacy of conservative 2–3 mm surgical margins for complete excision of biopsy-proven severely dysplastic nevi. Journal of the American Academy of Dermatology. https://doi.org/10.1016/j.jaad.2019.12.077
Ulgen, O., Yıldız, P., Acar, H., & Demirkesen, C. (2021). Analysis of interobserver reproducibility in grading dysplastic nevi: Results of the application of the 2018 World Health Organization grading criteria. Journal of Cutaneous Pathology, 49, 343–349. https://doi.org/10.1111/cup.14165
Vergara, R., Laharanne, E., De La Fouchardière, A., et al. (2025). Improving diagnostic accuracy in atypical melanocytic tumors using p16 immunohistochemistry and 9p21 fluorescence in situ hybridization: analysis of 206 second opinion cases. Scientific Reports, 15. https://doi.org/10.1038/s41598-025-95785-2
Wiedemeyer, K., Hartschuh, W., & Brenn, T. (2021). Dysplastic Nevi: Morphology and Molecular and the Controversies In-between. Surgical Pathology Clinics, 14(2), 341–357. https://doi.org/10.1016/j.path.2021.01.007